Morphologic Abnormalities
- Rectocele – bulging of the anterior rectal wall against the posterior vaginal wall.
Small rectoceles are frequent in asymptomatic women and may represent a normal variant.
Large rectoceles (> 2 cm) have a strong association with evacuation difficulty.
Rectoceles may contribute to passive leakage after incomplete evacuation.
Herniation of the pelvic peritoneal sac through the recto-genital space below de pubo-coccigeal ligament or recto-vaginal septum at the level or below the lower third of the vagina; it may contain fat (peritoneocele),
small bowel or a sigmoid segment (sigmoidocele).
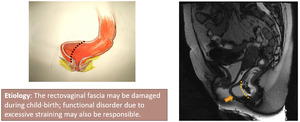
Fig. 47: Arrow - rectocele.
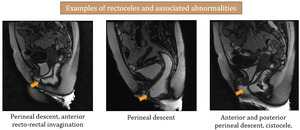
Fig. 48: Arrows - rectoceles
- Enterocele –Herniation of the pelvic peritoneal sac through the recto-genital space below de pubo-coccigeal ligament or recto-vaginal septum at the level or below the lower third of the vagina; it may contain fat (peritoneocele),
small bowel or a sigmoid segment (sigmoidocele).
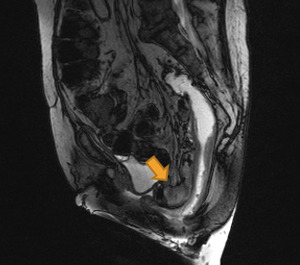
Fig. 33: Arrow - enterocele
Fig. 34: CINE RM. Enterocele formation during defecation.
- Cystocele - Bladder floor descent below the inferior border of the symphysis pubis (> 1 cm)
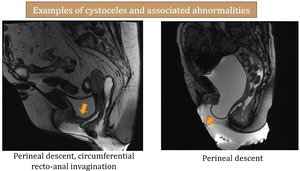
Fig. 35: Arrows - cystoceles
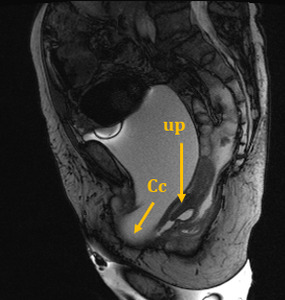
Fig. 36: Cc - cystocele, Up - uterine prolapse
Functional abnormalities
- Descending perineum / pelvic floor descent – excessive caudal movement of the pelvic floor during defecation.
Posterior compartment abnormality characterized by descent of the ano-rectal junction more than 3 cm below the PCL,
often associated with middle and anterior pelvic floor descent as well as rectocele,
intussusception,
organ prolapse and/or obstruction to defecation.
Pelvic floor descent is measured with the H line (normal diameter 5-6 cm).
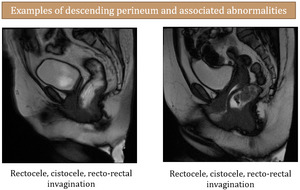
Fig. 24
- Intussusception and prolapse – defined as any organ descent beyond the H-line.
Rectal prolapse corresponds to a full thickness extrusion of the rectal wall beyond the anal verge.
On the other hand,
intussusception,
also termed internal rectal prolapse,
does not protrude through the anus,
but is confined to the rectum (intrarectal) or protrudes to the anal canal (intra-anal).
It is often associated with rectocele and/or enterocele,
and usually originates 6-8 cm above the anal verge,
where the main mucosal folds are located.
It is generally circumferential,
although it may have a focal presentation (often of the anterior rectal wall).

Fig. 25: Arrows - rectal intussusception
Left image - schematics of rectal intussusception
Middle Image - schematics of rectal prolapse
References: Jonas
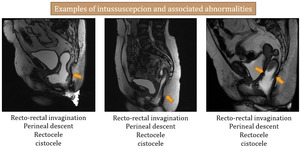
Fig. 37: Arrows - rectal intussusception
- Spastic pelvic syndrome /Dyskinetic Puborectalis / Anismus– inability of an abnormally contracted puborectalis to relax during defecation does not allow for a normal evacuation.
Anismus is a common cause of obstruction to defecation that is frequently overlooked.
It may be associated with pelvic floor descent and/or pubo-rectalis muscular hypertrophy.

Fig. 38: Arrow - persistence of pubo-rectalis muscle impression during defecation
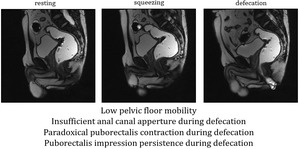
Fig. 39
- Paradoxical pubo-rectalis muscle contraction during defecation - associated with spastic pelvic syndrome

Fig. 40: Arrow - persistence of pubo-rectalis muscle impression during defecation
Fig. 50: CINE RM. Persistence of puborectalis muscle impression during defecation.
- Absent / insufficient anal canal aperture - associated withpelvic spastic syndrome

Fig. 41: CINE RM.
Spastic pelvic syndrome - the pelvic unit shows low mobility, the ano-rectal angle doesn't widen during defecation attempts and there is persistence of the pubo-rectalis muscle impression. Defecation was unsuccessful during examination.

Fig. 42: CINE RM.
Compared with the previous example, there is pelvic floor movement with perineal descent, formation of anterior rectocele and insufficient/absent apperture of the anal canal. Defecatory attempts are unsuccessful.
Case 1 – Fecal incontinence
- 88 year-old woman,
with rectal incontinence for soft stools and prolapse.
Images show an open anal canal at resting,
that widens during defecation,
associated with severe perineal descent,
rectal verticalization and prolapse,
uterine prolapse (it can be seen beyond the bladder at maximum defecatory effort) and cystocele.
The pelvic compartments are intricately related with each another.
This case illustrates multicompartment dysfunction that is most severe at the posterior segment,
with defecatory incontinence.
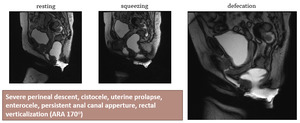
Fig. 29
Fig. 43: CINE RM - Defecatory phase
Case 2 – Posterior pelvic floor dysfunction
- 56 year-old woman,
with terminal obstipation
During defecation,
a significant rectocele is formed,
accompanied by perineal descent.
The anal canal has an insufficient apperture (< 5 mm).
These findings,
which are compatible with posterior pelvic floor dysfunction,
contribute to the obstruction to defecation that the patient complaints.
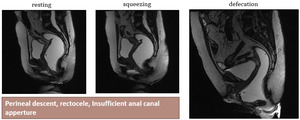
Fig. 30
Fig. 49: CINE RM . Defecatory phase.
MRI findings summary - what the clinican needs to know
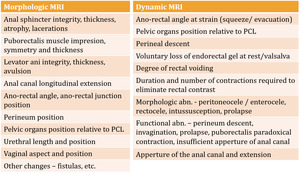
Fig. 31

